Extradural haematoma


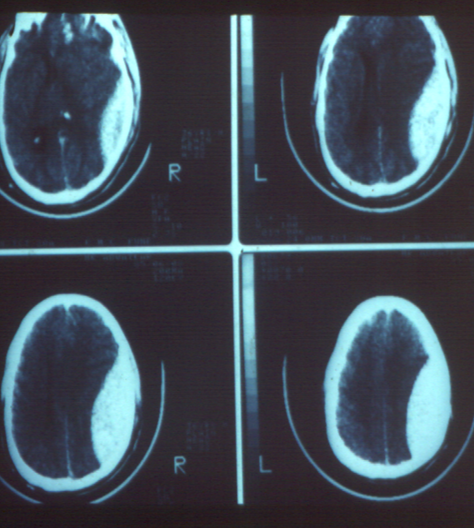
cerebral contusion causing severe brain injury
Management of head injuries
- Road Traffic Accidents (RTA) are a leading cause of head injury resulting in disability and death in India. The main reasons are poor infrastructure, unclear traffic regulations, poor implementation of rules, and safety measures, and population density. Other causes of head injury include falls from height, falling of heavy objects on the head and assault.
- Unfortunately, the victims are mainly the young males and breadwinners of the family. Early treatment is crucial to prevent secondary brain damage, which occurs when the initial impact triggers a cascade of processes that further damage the brain. The first hour of the head injury is called the Golden Hour where early aggressive treatment can save the brain from secondary and lasting damage. Ideally, this treatment should be started from the time the patient is transported in an ambulance.
- Severe head injuries result in an increase in intracranial pressure due to brain contusion, blood clot formation, and brain swelling. The situation gets worse due to low blood pressure from excessive bleeding caused by extensive scalp lacerations or injuries to other parts of the body. Treatment is aimed at controlling bleeding, securing the airway, providing oxygen, and maintaining blood pressure. Such a patient is best managed in a Neuro ICU.
- Once the patient is stabilized with primary treatment initial neurological examination and assessment of other injuries is done. The patient is transported for a CT scan of the brain and imaging of the spine, abdomen, and chest to rule out any other damages.
A Neurosurgeon is called at the site who does an assessment of the patient and CT scan and decides about further management.
Conditions requiring immediate surgery
1. Extensive scalp laceration- This can lead to significant blood loss and hypotension. The bleeding is controlled by suturing the scalp. Similarly, other areas of bleeding are attended to.
2. Penetrating injury and depressed fracture of the skull- Such injuries carry a high risk of infection in the brain and hence need early attention. The patient is taken to the operation theatre, the penetrating foreign body is removed and the depressed fracture is brought to its correct alignment. A thorough wash with normal saline and antibiotic solution is given to wash away contamination.
3. Extradural Haematoma- This is usually caused by a skull fracture injuring an underlying artery of the dura mater (outer covering of the brain) which is in close vicinity of the fractured site. This leads to rapid accumulation of blood clots on the surface of the dura mater under the skull, leading to acute compression of the brain, alteration of consciousness, and possible paralysis of limbs and coma. This life-threatening condition needs ultra-urgent surgical intervention. The patient is rushed to the operating room, the skull is trephined and blood clot is removed and the bleeding is controlled. The results of such treatment are very gratifying if performed in time. The patient who otherwise would have lost his/her life gains
 consciousness within hours and recovers without any loss of neurological functions.
consciousness within hours and recovers without any loss of neurological functions.
4. Brain contusion and Acute Subdural Haematoma- Severe injuries to the brain lead to contusion and laceration of the brain and sometimes rupture of bridging veins on the surface of the brain. This results in the accumulation of blood clots on the surface of the brain under the dura mater. The brain becomes tense leading to an increase in intracranial pressure and rapid deterioration in consciousness and often come. The patients have to be supported by a ventilator and treatment started with Mannitol, glycerol, etc. to reduce intracranial pressure. Such patients usually run a risk of brain stem compression due to herniation (shifting) of the brain. Immediate surgical intervention is needed by doing a large decompressive craniectomy. In this surgery, a large portion of the skull is lifted off and the dura mater is widely opened to allow the swollen brain to bulge outwards thus relieving the compressive effect from the brain stem. Results of this surgery are also gratifying provided the procedure is completed in time before any irreversible damage to the brain stem could take place.


Conditions requiring surgery at a later date-
1. Chronic Subdural Haematoma- This means slow development of blood collection under the dura mater and on the surface of the brain. A couple of weeks or months after a head injury the patient presents with symptoms of headache, drowsiness, imbalance, progressive paralysis, or mental changes. In elderly patients, there may not be any recollection of a significant head injury or they may recollect of a trivial trauma that was ignored. At the time of the head injury small quantity of blood clots is formed under the dura mater due to brain contusion or tear of a tiny bridging vein connecting to the dura. More blood clot and fluid start to collect around this and progressively increases in quantity eventually causing compression of the brain. The diagnosis is confirmed by a CT scan. This also needs immediate removal. Since the chronic subdural haematoma is a fluid haematoma they are easily drained through small trephine holes (burr holes). Again, the results are gratifying. In some cases, the patient wakes up from a coma immediately after or even during the surgery.
2. Cerebrospinal fluid leak - Cerebrospinal fluid (CSF) which is normally circulating in the brain finds its way to the nostrils (CSF rhinorrhoea) or ears (CSF otorrhoea) due to dura mater tear caused by a fracture at the base of the skull. Such leakages occur either immediately after the trauma or a few weeks or months later. Rarely CSF leak may occur even years after the accident. There is a risk of bacteria travelling retrograde into the brain through these defects and causing bacterial meningitis. Some patients come with meningitis years after a forgotten head injury that took place many years ago even during childhood. Surgical repair of dural tear by endoscopic transnasal route is recommended to prevent further episodes of meningitis.
3. Hydrocephalus- CSF which circulates in the brain finally comes to the surface of the brain to enter into a venous channel. In severe brain injuries due to contusions and cortical laceration, the CSF is unable to flow across the brain surface resulting in the accumulation of CSF. This back pressure results in dilatation of ventricles where the CSF is continuously forming. The resultant dilatation of the ventricles increases intracranial pressure. The patient presents with headache, imbalance, drowsiness, disorientation or memory loss. The treatment is aimed at diverting the accumulated CSF to other parts of the body. This is achieved by an operation called ventriculoperitoneal shunt where a silicon tube (biocompatible) of about 2 mm diameter is inserted into the ventricle through a small trephine in the skull and another tube is brought down after interposing a one-way valve to the abdomen under the skin and left inside the abdominal cavity. This drains CSF from the ventricles to the abdominal cavity in graduated quantity. Here again, the patient gets good relief from his/her symptoms.
Dr Dilip Kiyawat
Consultant Neurosurgeon
Jehangir Hospital, Pune
Penetrating injury to the brain